






| Total CBD: | 500 – 2500 mg |
| Potency: | 16.6 - 83.3 mg/mL |
| Cost per mg CBD: | $0.12 – $0.18 |
| Extract Type: | Full-spectrum |
| THC Content: | <0.3% |
Scroll to top
Evidence based
CBD for PMS: How It Helps with Cramps & Other Symptoms
Research has shown CBD oil can alleviate pain & cramping, support mood, & alleviate other common side effects of PMS.
Learn how it works, how much to take, and what side-effects to watch out for.

If you’re one of the 95% of women who experience premenstrual syndrome, it may come as a pleasant surprise that cannabidiol (CBD) may alleviate headaches, cramps, irritability, anxiety, insomnia and other annoying symptoms [1].
It’s not a magic cure-all, of course, but research shows that CBD may be effective as an anti-pain, anti-inflammatory, and anti-anxiety supplement.
One of the problems with PMS is that it’s extremely complex. Every woman (and every person) has slightly different hormone levels and a unique genetic makeup.
This article will cover everything you need to know about using CBD for premenstrual syndrome. We’ll cover how PMS works and what the current research suggests for supporting this condition.
Can CBD Oil Help With PMS?
PMS has a wide range of symptoms and involves the flux of two reproductive hormones — estrogen and progesterone.
CBD has little effect on these hormones directly but offers a variety of benefits that help alleviate symptoms involving pain, cramping, and mood.
The key benefits of CBD oil for PMS include:
- Relieves stress & anxiety symptoms
- Can help balance mood
- Alleviates pain
- Reduces nflammation
- Relaxes muscle tension & cramping
1. Relieves Stress & Anxiety Symptoms
CBD is considered a non-allosteric modulator — which is a fancy term that suggests it works by indirectly inhibiting certain activities in the brain. It uses the endocannabinoid system as the intermediary to stop the brain cells from firing, as opposed to allowing them to send signals.
While research on the endocannabinoid system is still being explored, this inhibitory behavior may explain why cannabidiol is known for being an anti-anxiety, anti-inflammatory, anti-convulsive, and anti-epileptic therapy [2].
2. May Help Balance Mood
While PMS is too complex of a topic for any single therapy to work as a cure-all, cannabidiol may be a good alternative to treat some of the symptoms related to serotonin — such as fluctuations in mood.
Since serotonin levels are thought to be affected by the changes in hormone levels during the luteal phase [3], cannabidiol’s interaction with serotonergic receptors may help relieve some of the symptoms arising from low serotonin levels [4].
Specifically, depression and anxiety are two negative emotional side effects that may benefit from taking cannabidiol through this interaction with serotonin.
3. Alleviates Pain
Cannabidiol has also been shown to relieve pain by blocking the signaling pathway for pain [5].
While the current research mainly focuses on cancer pain management and bone or joint problems (osteoarthritis), it isn’t too far of a stretch to think that cannabidiol may help relieve the muscle aches that happen as a result of PMS as well [6].
The endocannabinoid system regulates both the central and peripheral nervous systems. Since pain is transmitted via these nerves, ingesting cannabidiol has been shown in rats to help with reducing pain and inflammation [7].
Unfortunately, a review of clinical experiments in people shows conflicting results [8].
4. Reduces Inflammatory Load
Inflammation associated with premenstrual syndrome might also respond to cannabidiol.
However, inflammation is a complex immunological process involving many chemical cascades, feedback loops, and various cells from both the innate and the adaptive immune systems.
More research, specifically double-blind studies involving larger sample groups, need to be conducted to see if the cause of inflammation during PMS corresponds with the anti-inflammatory actions of cannabidiol [9, 10].
5. Alleviates Muscle Tension & Cramping
Most of the research on CBD and muscle has to do with treating spasticity in those with multiple sclerosis. Going back to the fact that CBD interacts with the endocannabinoid system and muscles are controlled by nerves, it is a logical step to think that CBD could have an effect on reducing muscle spasms [11].
Since the uterine cramping and spasms before and during menstruation, CBD, could in theory, affect and reduce cramping.
Related: How does CBD work for cramping?
What is PMS? What Causes It?
Premenstrual syndrome happens before the menstrual phase (hence the name). If you’re not familiar with the phases of the menstrual cycle, don’t worry, we’ll cover it in greater detail below.
PMS symptoms usually begin to develop after ovulation, within a week or so before menstruation.
Scientists aren’t able to say exactly why the change in hormones causes both the psychological and physical symptoms, but the theory is that it has something to do with the link between estrogen and serotonin production in the brain [12].
The entire menstrual cycle is a rollercoaster of hormones, each one taking their turn to rise up before crashing back down again. All of this is a well-choreographed dance designed to prepare the body for falling pregnant.
How Hormone Changes May Lead to PMS
- Progesterone and estrogen rise and then drop quickly after ovulation
- During this rise is when you start to feel physical symptoms such as breast tenderness. You can think of this as the body getting ready for pregnancy
- Because estrogen is tied to serotonin, the drop in estrogen causes a drop in serotonin as well
- Drops in serotonin (the neurotransmitter that makes you feel happy) can then cause the psychological symptoms

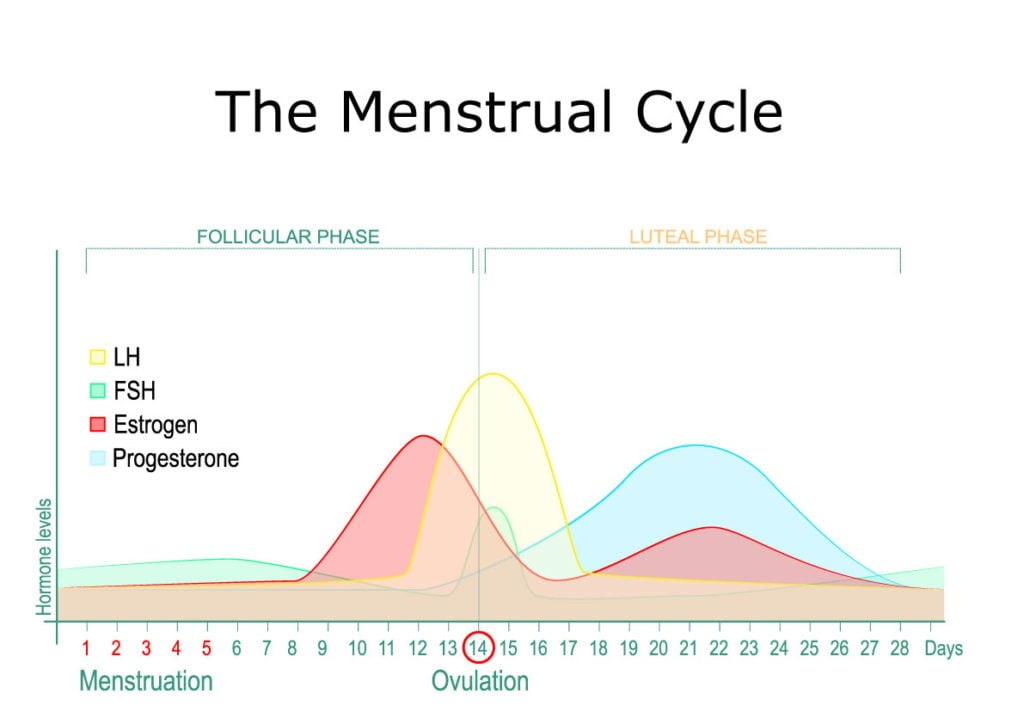
The 3 Stages of the Menstrual Cycle
The menstrual cycle can be broken down into 3 phases: follicular, luteal, and menses.
1. Follicular Phase
Eggs develop in little nests in the ovaries called follicles. During the follicular phase, the follicle that will eventually release a mature egg produces the hormone estrogen. This follicle is stimulated by a pituitary hormone called the Follicle Stimulating Hormone (FSH) [13].
FSH also stimulates the production of yet another pituitary gland hormone called Luteinizing Hormone (LH), which causes the egg to go through meiosis (cell division).
As estrogen levels rise with the growing follicle, the uterus lining thickens with tissue and blood vessels to get ready for implantation of a fertilized egg and pregnancy. Once the egg is mature, there is a spike in LH and the egg is released from the follicle — this marks the point of ovulation. The body is now ready to conceive a baby.
Estrogen, LH, and FSH levels begin to drop while progesterone starts to rise as it’s released from the same follicle that released the egg previously.
2. Luteal Phase
After ovulation is achieved during the follicular phase, we enter the luteal phase [14].
Here, estrogen rises again with progesterone and the uterus lining continues to grow. From the ovary, the egg will travel to the uterus via the fallopian tubes.
If fertilization were to occur, it would happen during this period of 3-4 days.
If no fertilization occurs, there’s no need to continue to support the highly vascularized and dense tissue of the uterus (using up a lot of the body’s resources). The corpus luteum dies and both estrogen and progesterone levels drop once again.
3. Menses or Menstruation
Menstruation is the process through which the cells lining the uterus go through programmed cell death (apoptosis) and shed [15].
Blood and tissue are expelled from the vagina and women may suffer from cramping which is the contraction of the uterine muscles to help shed the lining.
Signs & Symptoms of PMS
Because there are four different hormones at play here, PMS can present itself in various ways. Not all women get all the symptoms and not every symptom occurs every month. Jet lag, sleep, alcohol and smoking, and stress can all affect PMS.
Psychological Symptoms of PMS
The emotional changes that happen post-ovulation, during the luteal phase, may include the following:
- Depression
- Tension
- Anxiety
- Irritability
- Fatigue
- Emotional sensitivity
Physical Symptoms of PMS
Along with the changes in mood, physical symptoms will also occur.
These physical symptoms include:
- Breast tenderness
- Abdominal bloating
- Muscle and joint pain
- Headaches
- Inflammation [16]
- Cramping
Current Treatment Options for PMS
There are many ways to treat mild to severe PMS, including drugs, hormone therapy, acupuncture, hot packs, supplements, and much more.
The scientific evidence behind things like acupuncture is limited and most of the advice appears to be anecdotal [17]. Even exercise, a commonly suggested way to relieve PMS symptoms, showed inconsistent results when tested. Some groups responded while others showed no significant reduction in discomfort [18].
Hormonal options involve taking estradiol and/or progesterone pills in order to better regulate the fluctuations of these hormones in the luteal phase. Some studies have shown that this method is effective, while others showed no difference in alleviating the symptoms of PMS [19, 20].
What Else Can I Do To Relieve PMS Symptoms?
Aside from taking CBD, making sure to keep your serotonin levels at a normal level can help relieve PMS symptoms. Things like exercise, sleeping well, keeping stress levels low, and eating dark chocolate are all ways to make sure your serotonin level doesn’t dip too low.


Key Takeaways: Can CBD Help With PMS?
While the research on the use of cannabidiol on PMS symptoms still requires further exploration, the hope is that this article gave you a bit more insight into the causes of PMS and how CBD can be used to reduce PMS symptoms.
We know that CBD doesn’t directly treat PMS in its entirety. However, certain symptoms such as cramps, anxiety, and pain can somewhat be lessened by taking CBD.
Unlike other conditions, PMS symptoms and the severity of them vary month to month depending on the level of stress and other uncontrollable life issues that may arise unexpectedly. So, while it’s impossible to fully eliminate PMS due to its close ties with fluctuating reproductive hormones, it is possible to target particular symptoms on a case by case basis.
References Cited In This Article
- Kwan, I., & Onwude, J. L. (2015). Premenstrual syndrome. BMJ clinical evidence, 2015, 0806.
- Fernández‐Ruiz, J., Sagredo, O., Pazos, M. R., García, C., Pertwee, R., Mechoulam, R., & Martínez‐Orgado, J. (2013). Cannabidiol for neurodegenerative disorders: important new clinical applications for this phytocannabinoid?. British journal of clinical pharmacology, 75(2), 323-333.
- Shah, N. R., Jones, J. B., Aperi, J., Shemtov, R., Karne, A., & Borenstein, J. (2008). Selective serotonin reuptake inhibitors for premenstrual syndrome and premenstrual dysphoric disorder: a meta-analysis. Obstetrics and gynecology, 111(5), 1175–1182. doi:10.1097/AOG.0b013e31816fd73b
- National Academies of Sciences, Engineering, and Medicine. (2017). The health effects of cannabis and cannabinoids: the current state of evidence and recommendations for research. National Academies Press.Philpott, H. T., OʼBrien, M., & McDougall, J. J. (2017). Attenuation of early phase inflammation by cannabidiol prevents pain and nerve damage in rat osteoarthritis. Pain, 158(12), 2442–2451. doi:10.1097/j.pain.0000000000001052
- Blake A, Wan BA, Malek L, DeAngelis C, Diaz P, Lao N, Chow E, O’Hearn S. A selective review of medical cannabis in cancer pain management. Ann Palliat Med 2017;6(Suppl 2):S215-S222. doi: 10.21037/apm.2017.08.05
- Philpott, H. T., OʼBrien, M., & McDougall, J. J. (2017). Attenuation of early phase inflammation by cannabidiol prevents pain and nerve damage in rat osteoarthritis. Pain, 158(12), 2442–2451. doi:10.1097/j.pain.0000000000001052
- Häuser, W., Fitzcharles, M. A., Radbruch, L., & Petzke, F. (2017). Cannabinoids in Pain Management and Palliative Medicine. Deutsches Arzteblatt international, 114(38), 627–634. doi:10.3238/arztebl.2017.0627
- Gold, E. B., Wells, C., & Rasor, M. O. (2016). The Association of Inflammation with Premenstrual Symptoms. Journal of women’s health (2002), 25(9), 865–874. doi:10.1089/jwh.2015.5529
- Fernández-Ruiz, J., Sagredo, O., Pazos, M. R., García, C., Pertwee, R., Mechoulam, R., & Martínez-Orgado, J. (2013). Cannabidiol for neurodegenerative disorders: important new clinical applications for this phytocannabinoid?. British journal of clinical pharmacology, 75(2), 323–333. doi:10.1111/j.1365-2125.2012.04341.x
- Pozzilli, C. (2014). Overview of MS Spasticity. European Neurology, 71(s1), 1–3. doi: 10.1159/000357739
- Hofmeister, S., & Bodden, S. (2016). Premenstrual Syndrome and Premenstrual Dysphoric Disorder. American Family Physician, 94(3), 236–240. Retrieved from https://www.aafp.org/afp/2016/0801/p236.html
- Bowen, R. (2018). Gonadotropins: Luteinizing and Follicle Stimulating Hormones. Retrieved from http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/lhfsh.html
- Sohda, S., Suzuki, K., & Igari, I. (2017). Relationship Between the Menstrual Cycle and Timing of Ovulation Revealed by New Protocols: Analysis of Data from a Self-Tracking Health App. Journal of medical Internet research, 19(11), e391. doi:10.2196/jmir.7468
- Maybin, J. A., & Critchley, H. O. (2015). Menstrual physiology: implications for endometrial pathology and beyond. Human reproduction update, 21(6), 748–761. doi:10.1093/humupd/dmv038
- Gold, E. B., Wells, C., & Rasor, M. O. (2016). The Association of Inflammation with Premenstrual Symptoms. Journal of women’s health (2002), 25(9), 865–874. doi:10.1089/jwh.2015.5529
- Jang, S. H., Kim, D. I., & Choi, M. S. (2014). Effects and treatment methods of acupuncture and herbal medicine for premenstrual syndrome/premenstrual dysphoric disorder: systematic review. BMC complementary and alternative medicine, 14, 11. doi:10.1186/1472-6882-14-11
- Kroll-Desrosiers, A. R., Ronnenberg, A. G., Zagarins, S. E., Houghton, S. C., Takashima-Uebelhoer, B. B., & Bertone-Johnson, E. R. (2017). Recreational Physical Activity and Premenstrual Syndrome in Young Adult Women: A Cross-Sectional Study. PloS one, 12(1), e0169728. doi:10.1371/journal.pone.0169728
- Yonkers, K. A., Cameron, B., Gueorguieva, R., Altemus, M., & Kornstein, S. G. (2017). The Influence of Cyclic Hormonal Contraception on Expression of Premenstrual Syndrome. Journal of women’s health (2002), 26(4), 321–328. doi:10.1089/jwh.2016.5941
- Naheed, B., Kuiper, J. H., Uthman, O. A., O’Mahony, F., & O’Brien, P. M. (2017). Non-contraceptive oestrogen-containing preparations for controlling symptoms of premenstrual syndrome. The Cochrane database of systematic reviews, 3(3), CD010503. doi:10.1002/14651858.CD010503.pub2
More Health Conditions to Explore
-
Conditions Related to Health Benefits
- CBD For Allergies: Can This Cannabinoid Ease Symptoms?
- Top 10 CBD Oils For Back Pain
- Can CBD Help With Menstrual Cramps?
- CBD for Sciatica: How It Works, Safety, Drug Interactions, & Best Products
- Is CBD a Viable Treatment for Cerebral Palsy?
- CBD Oil For Sleep
- CBD For Psoriasis: Can CBD Help to Alleviate Symptoms?
- Traumatic Brain Injury (TBI)
- Arthritis
- Anxiety & Depression
- Weight Loss
- ADD & ADHD
- Anorexia
- Alzheimer’s Disease & Dementia
- Addiction
- ALS (Amyotrophic Lateral Sclerosis)
- Antibiotic Resistance
- Asthma
- Atherosclerosis
- Autism
- Acne
- Bipolar Disorder
- Pain
- Crohn's Disease & Ulcerative Colitis
- Diabetes
- Epilepsy
- Endocrine Disorders
- Fibromyalgia
- Fatty Liver Disease
- Glaucoma
- Hypertension
- Heart Disease
- Huntington's Disease
- Inflammation
- Irritable Bowel Syndrome (IBS)
- Kidney Disease
- Migraine Headaches
- Muscle Recovery
- Multiple Sclerosis
- Motion Sickness
- Metabolic Syndrome
- Neurodegeneration
- Cancer
- Nausea
- Neuropathic (Nerve) Pain
- Osteoporosis/Bone Health
- Obsessive-Compulsive Disorder (OCD)
- Polycystic Ovarian Syndrome (PCOS)
- PTSD
- Prion/Mad Cow Disease
- Premenstrual Syndrome (PMS)
- Parkinson’s Disease
- Schizophrenia
- Sickle Cell Anemia
- Stroke
-
Conditions Related to Products
- Ranking The Top 13 THC Gummies By Category (Δ8, Δ9, Δ10, HHC, & More)
- Top 10 CBD Oils For Back Pain
- Everything You Need to Know About CBD Sunscreen
- Top 7 CBD Gummies For Sleep & Insomnia
- Top 7 CBD Gummies To Help With Anxiety (2022)
- Best CBD Gummies For Pain (Top-Rated Pain Gummies For 2022)
- Best Hemp Cigarettes (Top 5 Nicotine-Free Smokes)
- Top 5 CBD Lip Balms For 2022
- The Top 7 CBD Face Masks for 2022
- The Best CBD Inhalers For 2022 (& How to Use Them)
- Best Full-Spectrum CBD Vape Juice: What to Look For & How to Use It
- CBD Eye Drops: New Option For Glaucoma?
- CBD Oil For Dogs With Arthritis
- Best CBD Massage Oils In 2022
- Buyer's Guide To The Best CBD Vape Kits In 2022
- CBD Chocolate: Yes, It Exists & It's Just as Divine as it Sounds
- CBD Pre-Rolls & Cigarettes
- Terpene Concentrates
- Best CBD Soaps
- Best CBD Shampoo & Conditioner
- Best CBD Juul Pods
- CBD Isolate Oils
- Full-Spectrum CBD Oils
- Best CBD Lube
- CBD Honey
- CBD Transdermal Patches
- Best Dry Herb Vaporizers
- CBD Oil For Dogs With Epilepsy
- CBD Oil For Dogs With Anxiety
- CBD Oil For Dogs With Cancer
- CBD For Horses
- CBD Chewing Gum
- CBD Pain Cream
- CBD Oil For Cats
- CBD Oil For Dogs
- CBD Hemp Flower
- CBD Suppositories
- Best CBD Gummies for Pain, Sleep & Anxiety Reviewed (2022)
- CBD Teas
- CBD Vape Pens
- CBD Vape Oils
- CBD Coffee
- CBD Drinks & Shots
- CBD Crystals
- CBD Skincare
- Best CBD Oil & Gummies For Kids: Is CBD Safe for Children with Anxiety & ADHD?
- CBD Concentrates
- CBD Bath Bombs
- CBD Capsules
- CBD Sprays
- CBD Dog Treats
-
Conditions Related to Topicals
-
Conditions Related to Oils & Tinctures
-
Conditions Related to Edibles
- Top 7 CBD Gummies To Help With Anxiety (2022)
- Best CBD Gummies For Pain (Top-Rated Pain Gummies For 2022)
- CBD Chocolate: Yes, It Exists & It's Just as Divine as it Sounds
- CBD Honey
- CBD Chewing Gum
- Best CBD Gummies for Pain, Sleep & Anxiety Reviewed (2022)
- CBD Teas
- CBD Coffee
- CBD Drinks & Shots
- CBD Capsules
-
Conditions Related to Gummies
- Ranking The Top 13 THC Gummies By Category (Δ8, Δ9, Δ10, HHC, & More)
- Top 7 CBD Gummies For Sleep & Insomnia
- Top 7 CBD Gummies To Help With Anxiety (2022)
- Best CBD Gummies For Pain (Top-Rated Pain Gummies For 2022)
- Best CBD Gummies for Pain, Sleep & Anxiety Reviewed (2022)
- Best CBD Oil & Gummies For Kids: Is CBD Safe for Children with Anxiety & ADHD?
-
Conditions Related to Hemp Flower
-
-
Conditions Related to Terpenes
-
-
Conditions Related to Cultivation
-
Conditions Related to Concentrates
-
Conditions Related to Delta 8 THC
-
Conditions Related to Delta 9 THC
-
-
-
-
Conditions Related to CBD
- Everything You Need to Know About CBD Sunscreen
- Top 7 CBD Gummies For Sleep & Insomnia
- Top 7 CBD Gummies To Help With Anxiety (2022)
- Best CBD Gummies For Pain (Top-Rated Pain Gummies For 2022)
- Best Hemp Cigarettes (Top 5 Nicotine-Free Smokes)
- Top 5 CBD Lip Balms For 2022
- The Top 7 CBD Face Masks for 2022
- The Best CBD Inhalers For 2022 (& How to Use Them)
- Best Full-Spectrum CBD Vape Juice: What to Look For & How to Use It
- CBD Eye Drops: New Option For Glaucoma?
- CBD Oil For Dogs With Arthritis
- Best CBD Massage Oils In 2022
- Buyer's Guide To The Best CBD Vape Kits In 2022
- CBD Chocolate: Yes, It Exists & It's Just as Divine as it Sounds
- CBD Pre-Rolls & Cigarettes
- Best CBD Soaps
- Best CBD Shampoo & Conditioner
- Best CBD Juul Pods
- CBD Isolate Oils
- Full-Spectrum CBD Oils
- Best CBD Lube
- CBD Honey
- CBD Transdermal Patches
- CBD Oil For Dogs With Epilepsy
- CBD Oil For Dogs With Anxiety
- CBD Oil For Dogs With Cancer
- CBD For Horses
- CBD Chewing Gum
- CBD Pain Cream
- CBD Oil For Cats
- CBD Oil For Dogs
- CBD Hemp Flower
- CBD Suppositories
- Best CBD Gummies for Pain, Sleep & Anxiety Reviewed (2022)
- CBD Teas
- CBD Vape Pens
- CBD Vape Oils
- CBD Coffee
- CBD Drinks & Shots
- CBD Crystals
- CBD Skincare
- Best CBD Oil & Gummies For Kids: Is CBD Safe for Children with Anxiety & ADHD?
- CBD Concentrates
- CBD Bath Bombs
- CBD Capsules
- CBD Sprays
- CBD Dog Treats
-
-
Conditions Related to THC-O
-
-


Conditions Related to Joint Health
-


Conditions Related to Pain Disorders
- Top 10 CBD Oils For Back Pain
- Can CBD Help With Menstrual Cramps?
- CBD for Sciatica: How It Works, Safety, Drug Interactions, & Best Products
- Traumatic Brain Injury (TBI)
- Arthritis
- Pain
- Fibromyalgia
- Glaucoma
- Inflammation
- Kidney Disease
- Migraine Headaches
- Multiple Sclerosis
- Neuropathic (Nerve) Pain
- Premenstrual Syndrome (PMS)
- Sickle Cell Anemia
-

Conditions Related to Autoimmune Disease
-

Conditions Related to Cognitive Health
-

Conditions Related to Metabolic Disorders
-


Conditions Related to Psychological Disorders
-


Conditions Related to Muscles & Bones
-


Conditions Related to Nervous System
- CBD for Sciatica: How It Works, Safety, Drug Interactions, & Best Products
- Is CBD a Viable Treatment for Cerebral Palsy?
- CBD Oil For Sleep
- Traumatic Brain Injury (TBI)
- Anxiety & Depression
- ADD & ADHD
- Anorexia
- Alzheimer’s Disease & Dementia
- Addiction
- ALS (Amyotrophic Lateral Sclerosis)
- Autism
- Bipolar Disorder
- Epilepsy
- Huntington's Disease
- Inflammation
- Migraine Headaches
- Multiple Sclerosis
- Motion Sickness
- Neurodegeneration
- Neuropathic (Nerve) Pain
- Obsessive-Compulsive Disorder (OCD)
- PTSD
- Prion/Mad Cow Disease
- Parkinson’s Disease
- Schizophrenia
-


-

Conditions Related to Reproductive Health
-


Conditions Related to Hormones & Endocrine
-


Conditions Related to Skin Health
-


Conditions Related to Cardiovascular System
-


Conditions Related to Digestive System
-


Conditions Related to Genetic Disorders
-

Conditions Related to For Children














Trending Articles


User Guide, CBD, Dosage
CBD Dosage Calculator: How Much CBD Should I Take?


Cannabinoids, CBG
CBG (Cannabigerol): The Cannabis Stem Cell

User Guide, CBD, CBD Oil, Terpenes
Full-Spectrum CBD Oil vs. CBD Isolate: What’s the Difference?


User Guide, Resources, Legal, Cannabis Flower
Hemp vs. Marijuana: What’s the Difference?



Reviews, User Guide, CBD, CBD Oil, Legal
Scam CBD Companies You Should Probably Stay Away From

User Guide, For Parents, CBD, Side Effects, CBD Oil
What Are The Side Effects of CBD?
User Guide, Pets, CBD Oil
Yes, You Can Give Your Pets ‘Human’ CBD Oil
Trending Articles
User Guide, CBD, Dosage
CBD Dosage Calculator: How Much CBD Should I Take?
Cannabinoids, CBG
CBG (Cannabigerol): The Cannabis Stem Cell
User Guide, CBD, CBD Oil, Terpenes
Full-Spectrum CBD Oil vs. CBD Isolate: What’s the Difference?
User Guide, Resources, Legal, Cannabis Flower
Hemp vs. Marijuana: What’s the Difference?
Reviews, User Guide, CBD, CBD Oil, Legal
Scam CBD Companies You Should Probably Stay Away From
User Guide, For Parents, CBD, Side Effects, CBD Oil
What Are The Side Effects of CBD?