









Scroll to top

Evidence based
What is the Endocannabinoid System?
Most of the benefits of CBD relies on the endocannabinoid system.
Here’s how it works & what can happen if it isn’t working correctly.

Cannabis wouldn’t offer us any benefit if it weren’t for the endocannabinoid system — or ECS for short.
The medicinal benefits of CBD mainly rely on its ability to regulate this key system — which is involved with everything from mood and sleep support to pain transmission and neurological function.
The ECS was only discovered in the late 1980s and early 90s. We still only have a basic understanding of how this system works and how it’s involved in human health and disease.
Here, we’ll cover the ECS at length. We’ll discuss each of the system’s core components, how cannabinoids like THC and CBD interact with it, and what recent advances in medical research have uncovered about the role of ECS in illness.
What is the Endocannabinoid System (ECS)?
The endocannabinoid system (ECS) is a complex cell-signaling system. It’s used to regulate a wide range of functions around the body, including hormone regulation, body temperature, sleep, mood, and much more.
Cannabinoids from the cannabis plant (such as THC and CBD) work by interacting with this system. The endocannabinoid system is always active, even if you don’t use or have never used cannabis products.
The ECS was discovered in the 1990s, but to this day, science only has a basic understanding of how it works and what its specific role is in the human body.
We know that the ECS is present in all life on earth with a central nervous system and that it’s essential for maintaining the internal balance of the body (called homeostasis). When something forces the body out of balance, such as an injury, starvation, or stress, the ECS steps in to help us find balance again.
Due to its diverse and critically important role in the body, there’s a lot of potential for developing new medicines that leverage this critical system. Many of the conditions being explored were previously considered untreatable [1] (more on this later).
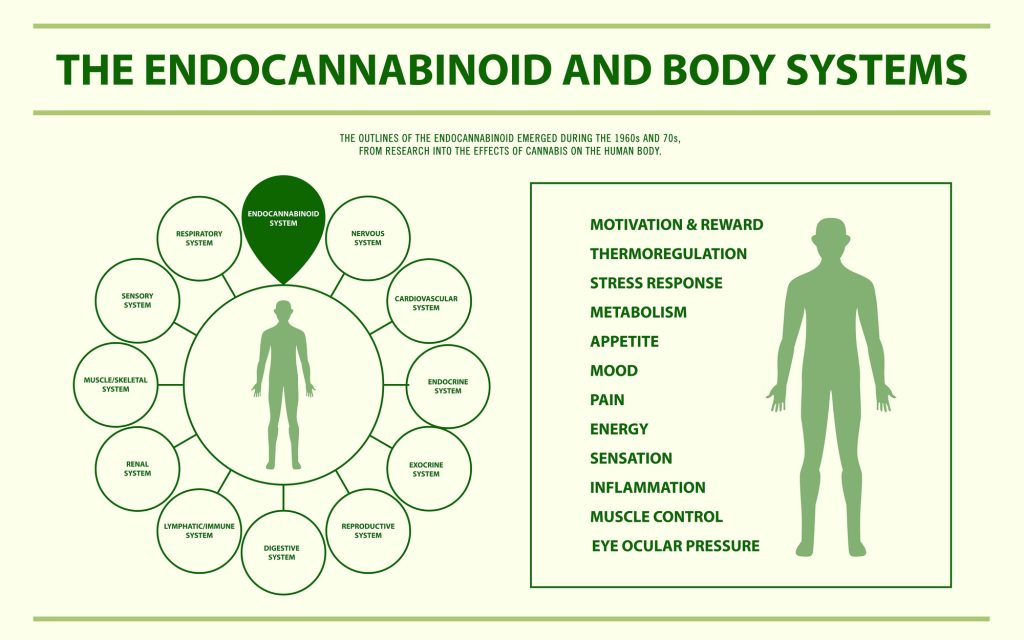
What Does the Endocannabinoid System Do?
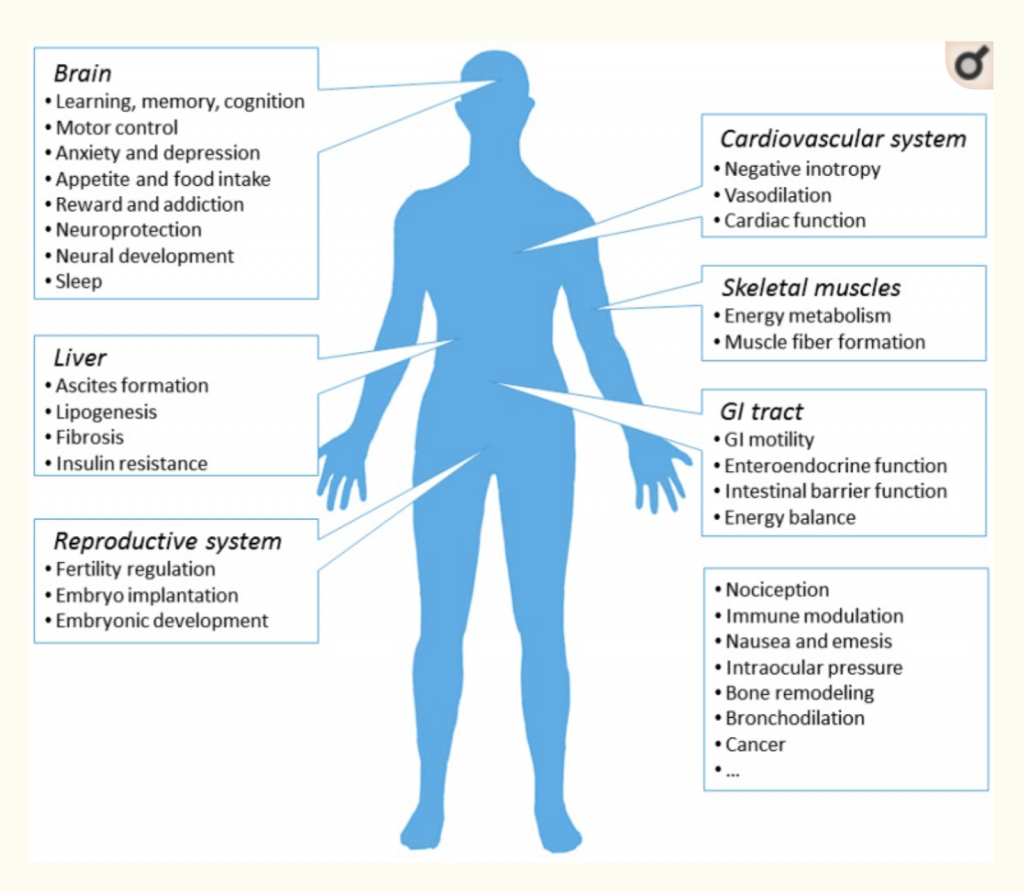
The ECS does a surprising amount of things for the body. Despite how little we know about this system, we know that it’s essential for just about every organ system in the body in one way or another.
Explaining exactly what this system does is difficult because, unlike other body systems, it doesn’t just have one function. It’s involved with tens, if not hundreds, of individual cell functions. Studies have shown that the ECS is involved with controlling when we feel hungry when we feel sleepy, and when our immune system should sound the alarms or when it should relax.
But what exactly is the ECS actually doing? How does it offer so many different functions?
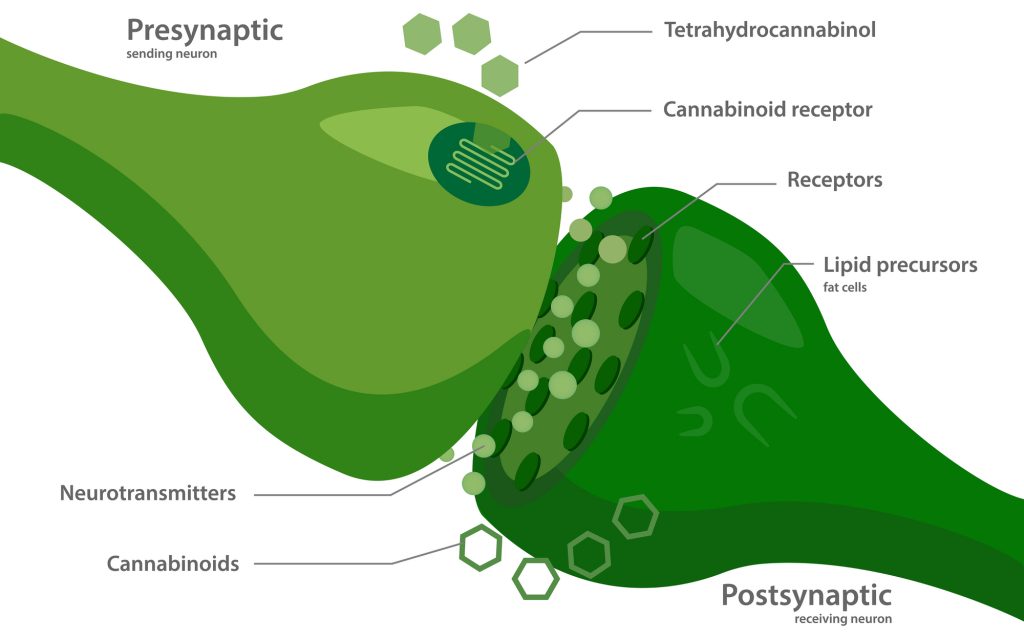
The ECS acts as a facilitator for the nervous system. If you remember from 8th-grade biology, the nervous system transmits information around the body — telling your organs what to do and when to do it. Without this system, each of our internal organs wouldn’t work together as a whole.
The ECS is an integral part of this system by acting as the “read-receipts” for the nervous system. It performs what’s called “retrograde signaling” — which means the signal is sent in the opposite direction (just like a read-receipt).
The nerve cells transmit a signal from the brain to a specific organ or vice versa. The ECS then sends a message in reverse to let the sender know the message was received.
This may seem trivial, but it has enormous implications on how our internal organs work together and function as a whole. When the ECS isn’t working properly, we experience all sorts of problems, as we’ll cover later in this article. A few examples are conditions like fibromyalgia, irritable bowel syndrome, or migraine headaches. It can also affect our ability to resist or manage stress effectively, make us less fertile, negatively impact our sleep, and may even lead to autoimmune disease.
Functions of the Endocannabinoid System:
- Sleep
- Motor control (movement & muscle coordination)
- Heart health
- Mood
- Learning & memory
- Pain regulation
- Appetite
- Bone growth & remodeling
- Metabolism
- Liver function
- Stress
- Reproduction
- Skin & connective tissue health
The Three Components of the Endocannabinoid System
- The endocannabinoid receptors — the part of the system that performs the action
- The endocannabinoids — tells the receptors what to do
- Enzymes — this part disposes of the endocannabinoids once they’re no longer needed
1. The Endocannabinoid Receptors
(The part that performs the action)
The endocannabinoid receptors are found on just about every cell of the human body. This is the part of the system that exerts the effect. When they become active, they cause a change in the cell.
There are two different types of endocannabinoid receptors:
- CB1 Receptors — Primarily found in the central nervous system (spinal cord and brain). They’re involved with regulating the digestive mobility, secretion of gastric fluids, neurotransmitter and hormone function, intestinal permeability, appetite, mood regulation, and more [3].
- CB2 Receptors — Primarily found outside the central nervous system. They’re abundant in the internal organs, peripheral nervous system (the nerve cells located outside the brain and spinal cord), and immune cells.
There are also a couple of other receptors involved with this system that aren’t directly considered endocannabinoid receptors. This includes the TRP receptors (vanilloid receptors) and peroxisome proliferator-activated receptors (PPARs). They’re considered to be involved because endocannabinoid messengers interact with them, but they serve separate functions.
2. The Endocannabinoids
(The messengers that tell receptors what to do and when to do it)
The endocannabinoids are the chemical messengers (eicosanoids) designed to interact with the endocannabinoid receptors. They’re used to transmit messages from one part of the body to another, telling the endocannabinoid receptors what to do.
There are two endocannabinoids. Each one has slightly different roles:
- Arachidonylethanolamide (Anandamide) — primarily involved with the ECS located outside the brain and spinal cord.
- 2-arachidonoylglycerol (2-AG) — primarily involved with the ECS located inside the brain and spinal cord. THC closely resembles the shape of 2-AG.
3. Endocannabinoid Enzymes
(The part that removes the endocannabinoids when they’re no longer needed)
Enzymes are a specific type of protein that breaks down chemicals in the body. There are two types of enzymes that are responsible for breaking down each of the endocannabinoids. They act like a garbage disposal. Once a message is received, the messenger is broken down and destroyed.
Without these enzymes, the endocannabinoids would continue to accumulate and cause too much activity at the endocannabinoid receptor sites.
Endocannabinoid enzymes include:
- Fatty Acid Amide Hydrolase (FAAH) — this enzyme breaks down anandamide
- Monoacylglycerol Acid Lipase (MAGL) — this enzyme breaks down 2-AG
Endocannabinoid System Diagram
When Was the Endocannabinoid System Discovered?
The endocannabinoid system was first discovered by a group of researchers funded by the United States government in 1988 [2]. They found a unique receptor type that responded to a cannabis extract. What they had found at this time were the CB1 endocannabinoid receptors.
After this discovery, research on the endocannabinoid system exploded. A team at Pfizer pharmaceuticals created an analog of THC that allowed researchers to radioactively tag and map the location of these receptors. This lead to the discovery that the endocannabinoid receptors were far more abundant in the brain than any other neurotransmitter type. It also helped researchers discover the second type of endocannabinoid receptor — called the CB2 receptors.
In 1992, the work of three researchers, Raphael Mechoulam, William Devane, and Dr. Lumir, discovered a naturally occurring chemical messenger that interacted with the endocannabinoid receptors. What these researchers discovered was eventually named anandamide (derived from the Sanskrit word for “bliss”).
After this point, researchers discovered that the endocannabinoid system has a specific function in the body and wasn’t there solely for the purpose of responding to THC. Three years later, Mechoulam and his team discovered the second endocannabinoid — 2-AG.
Since these discoveries, scientists have been working to understand all the nuances involved with this system, how it works, and its relevance in human health and wellbeing. We still have a long way to go in this field of research.

The Endocannabinoid System & Cannabis
Any cannabinoid that comes from plant sources is referred to as phytocannabinoids (phyto- referring to plant-based sources).
Conversely, cannabinoids produced inside the body are referred to as endocannabinoids (endo- meaning “inside the body”).
Cannabis is the most potent and diverse source of compounds able to interact with the endocannabinoid system.
A cannabinoid, by definition, is any compound that can interact with the endocannabinoid system. Some directly stimulate the ECS receptors (like THC), others bind to it without activating them (like CBD), and some even block its effects. Others work by blocking the enzymes responsible for breaking down endocannabinoids like anandamide or 2-AG.
THC makes us feel high by stimulating endocannabinoid receptors in the brain that are involved with regulating serotonin. Others are more useful for stimulating or inhibiting appetite, and some are involved with immune function or the stress response.
CBD (Cannabidiol)
Cannabidiol is the primary active ingredient in both marijuana and hemp that offers the majority of the medicinal benefits. This cannabinoid is non-psychoactive, which means it doesn’t make users feel high.
This compound doesn’t directly stimulate the endocannabinoid receptors. Instead, it supports the function of our naturally occurring endocannabinoids. It competes for the enzymes that break down anandamide (FAAH), causing our anandamide levels to increase.
Some research suggests CBD may exert many of its actions by binding to a new endocannabinoid receptor that hasn’t been discovered yet.
This system is extremely complex. Despite decades of research conducted by the greatest minds in the field, we still only have a rudimentary understanding of how CBD actually works.
CBDV (cannabidivarin) is another closely related analog of CBD found predominantly in African landrace strains of cannabis. This cannabinoid has much less research available but appears to share similar effects on the endocannabinoid system.
THC (Tetrahydrocannabinol)
Delta 9 THC is the primary cannabinoid in marijuana that makes users feel high. The characteristic changes in perception and emotion result from this ingredient’s interaction with the endocannabinoid system.
Delta 9 THC stimulates both the CB1 and CB2 endocannabinoid receptors.
Activating these receptors causes several changes in the body. It increases appetite, stimulates immune activity, and causes a cascade of effects in the brain that lead to the effects we experience while we’re high. This includes euphoria, auditory and visual perception changes, alterations in our interpretation of time, and more. The main cause of this is thought to be the activation of the 5-HT2A receptors caused by CB1 receptor activity in the brain’s prefrontal cortex.
There are three other versions of this compound as well — delta 7 THC, delta 8 THC, and delta 10 THC — but these compounds are about 50% as potent and are only found in trace amounts in the cannabis plant.
Another version, called HHC (hydroxyhexahydrocannabinol) has roughly the same affinity for the endocannabinoid receptors, but the chemical structure is much more stable. This gives HHC an exceptionally long shelf-life.
THCP (tetrahydrocannabiphorol) can also be found in delta 7, 8, 9, or 10 isomers, but is differentiated by its extra-long alkyl side chain. This long side-chain gives THCP nearly 33 times higher affinity for binding to the CB1 endocannabinoid receptors.
There are also synthetic forms of THC that have powerful CB1 and CB2 agonistic activity. One of the most popular versions today is THC-O-acetate — which serves as a more bioavailable prodrug of THC.
CBC (Cannabichromene)
Cannabichromene is the third most abundant cannabinoid in the cannabis plant. What makes this cannabinoid different from the rest is that it doesn’t have much affinity for binding to either of the endocannabinoid receptors. Instead, it has a strong affinity for the related TRPV receptors.
CBG (Cannabigerol)
Cannabigerol is the precursor to CBD, THC, and CBC, depending on which enzymes are present in the plant. This cannabinoid interacts with the CB1 and CB2 receptors in a similar way as CBD, but with less of an impact.
CBN (Cannabinol)
Cannabinol is formed when THC breaks down. This phytocannabinoid’s chemical structure is only slightly different and therefore has a similar interaction with the endocannabinoid system. CBN binds to both the CB1 and CB2 receptors just like THC. However, it has significantly less potency — only causing about 10% of the strength as THC.
CBN is technically psychoactive for this effect, but it’s so weak it’s unlikely to cause any noticeable changes.
THCV (Tetrahydrocannabivarin)
THCV is considered a neutral agonist (stimulates) for both the CB1 and CB2 receptors. This means it binds to the receptors but doesn’t exert much of an impact. Some reports suggest THCV is about 25% as strong as THC in terms of its psychoactive effects — but this is also disputed. More research is needed to understand the role of THCV on the endocannabinoid system in greater detail.

The Endocannabinoid System & Disease
We know the ECS has a major impact on our physical health and wellbeing — so it makes sense that if there’s a problem with this system, it can lead to illness.
With that said, it’s not clear what role the ECS has in human pathology. This system is so complex it’s difficult to pinpoint exactly what’s going on when the ECS isn’t working properly.
Endocannabinoid Deficiency
Scientists have put forward a theory that certain medical conditions may be caused by deficiency or dysfunction of the endocannabinoid system. This condition has been dubbed clinical endocannabinoid deficiency (CED). This theory could explain an underlying cause for a variety of idiopathic medical conditions.
Idiopathic is a term that refers to medical conditions or symptoms that don’t have any identifiable causes. A few examples include migraine headaches, fibromyalgia, and irritable bowel syndrome. None of these conditions have a good explanation for what causes them. There Are plenty of theories, but nothing so far has done a great job at explaining what causes them thus far.
The conventional medical system usually refers to these conditions as being “psychosomatic” — which essentially means they’re caused by the mind, rather than any physical causes. This, of course, makes it extremely difficult to treat these conditions. And it’s true; there are very few medical treatments available for these conditions. Most people diagnosed with these disorders will continue to live with them for the rest of their lives.
The endocannabinoid deficiency theory is a promising candidate for all of these conditions — as pointed out in a 2016 article by prominent cannabis researcher Ethan Russo [5].
Other conditions have also been suggested to have endocannabinoid dysfunction at its origins — such as Alzheimer’s disease, Parkinson’s disease, and depression.
None of these theories have been proven. But they haven’t been disproven yet either. We simply need more research to understand what’s going on here and whether or not the ECS is truly at the root of these perplexing diseases.
Potential Signs of Endocannabinoid Deficiency:
- Poor digestive function
- Mood disorders or instability
- Disruptions in sleep patterns
- Increased sensitivity to pain
- Failure to thrive
- Autoimmune dysfunction
What Causes Endocannabinoid Deficiency?
- Genetic disorders
- Stunted development in early childhood
- Viral infection
Conditions That May Be Linked to CED
- Post Traumatic Stress Disorder (PTSD) [4]
- Irritable bowel syndrome (IBS) [5]
- Migraine headaches [5]
- Fibromyalgia [5]
- Neonatal failure to thrive [6]
- Cystic fibrosis [7]
- Brachial plexopathy [8]
- Causalgia [9]
- Glaucoma [10]
- Dysmenorrhea [11]
- Phantom limb pain
- Hyperemesis gravidarum [12]
- Repetitive miscarriages
- Bipolar Disorder [13]
- Huntington’s disease [14]
- Multiple Sclerosis [15]
- Motion sickness [16]
- Parkinson’s disease [17]
Summary: What is the ECS?
The ECS has baffled researchers for decades. Since its discovery in the late 80s, science has discovered this system is involved in just about every organ system in the human body — some much more than others. There are more ECS receptors in the human brain than any other neurotransmitter type.
Despite how important this system is for maintaining our overall health and wellbeing, we know surprisingly little about it.
What we do know is that cannabinoids like CBD and THC offer the majority of their benefits by regulating this core system. This is what allows these compounds to treat conditions that were otherwise considered “untreatable”.
This is a rapidly evolving space. Every year research unlocks new insights into how the ECS works within the body, its role in human disease, and how various plant and man-made chemicals interact with this system to provide medicinal or recreational benefits. Sign up for our newsletter below to stay up to date on new developments in this space.
Endocannabinoid System Research
- Pacher, P., Bátkai, S., & Kunos, G. (2006). The endocannabinoid system as an emerging target of pharmacotherapy. Pharmacological Reviews, 58(3), 389-462.
- Devane, W. A., Dysarz, F. 3., Johnson, M. R., Melvin, L. S., & Howlett, A. C. (1988). Determination and characterization of a cannabinoid receptor in rat brain. Molecular Pharmacology, 34(5), 605-613.
- Zou, S., & Kumar, U. (2018). Cannabinoid receptors and the endocannabinoid system: signaling and function in the central nervous system. International journal of molecular sciences, 19(3), 833.
- Marsicano, G., Wotjak, C. T., Azad, S. C., Bisogno, T., Rammes, G., Cascio, M. G., … & Di Marzo, V. (2002). The endogenous cannabinoid system controls extinction of aversive memories. Nature, 418(6897), 530-534.
- Russo, E. B. (2016). Clinical endocannabinoid deficiency reconsidered: current research supports the theory in migraine, fibromyalgia, irritable bowel, and other treatment-resistant syndromes. Cannabis and cannabinoid research, 1(1), 154-165.
- Fride, E., Bregman, T., & Kirkham, T. C. (2005). Endocannabinoids and food intake: newborn suckling and appetite regulation in adulthood. Experimental Biology and Medicine, 230(4), 225-234.
- Fride, E. (2002). Cannabinoids and cystic fibrosis: a novel approach to etiology and therapy. Journal of Cannabis Therapeutics, 2(1), 59-71.
- Berman, J. S., Symonds, C., & Birch, R. (2004). Efficacy of two cannabis-based medicinal extracts for relief of central neuropathic pain from brachial plexus avulsion: results of a randomised controlled trial. Pain, 112(3), 299-306.
- Notcutt, W., Price, M., Miller, R., Newport, S., Phillips, C., Simmons, S., & Sansom, C. (2004). Initial experiences with medicinal extracts of cannabis for chronic pain: results from 34 ‘N of 1’studies. Anaesthesia, 59(5), 440-452.
- Järvinen, T., Pate, D. W., & Laine, K. (2002). Cannabinoids in the treatment of glaucoma. Pharmacology & Therapeutics, 95(2), 203-220.
- Russo, E. (2002). Cannabis treatments in obstetrics and gynecology: a historical review. Journal of Cannabis Therapeutics, 2(3-4), 5-35.
- Westfall, R. E., Janssen, P. A., Lucas, P., & Capler, R. (2006). Survey of medicinal cannabis use among childbearing women: patterns of its use in pregnancy and retroactive self-assessment of its efficacy against ‘morning sickness.’ Complementary Therapies in Clinical Practice, 12(1), 27-33.
- Ashton, C. H., Moore, P. B., Gallagher, P., & Young, A. H. (2005). Cannabinoids in bipolar affective disorder: a review and discussion of their therapeutic potential. Journal of Psychopharmacology, 19(3), 293-300.
- Bisogno, T., Martire, A., Petrosino, S., Popoli, P., & Di Marzo, V. (2008). Symptom-related changes of endocannabinoid and palmitoylethanolamide levels in brain areas of R6/2 mice, a transgenic model of Huntington’s disease. Neurochemistry international, 52(1-2), 307-313.
- Baker, D., Pryce, G., Croxford, J. L., Brown, P., Pertwee, R. G., Makriyannis, A., … & Marzo, V. D. (2001). Endocannabinoids control spasticity in a multiple sclerosis model. The FASEB Journal, 15(2), 300-302.
- Choukèr, A., Kaufmann, I., Kreth, S., Hauer, D., Feuerecker, M., Thieme, D., … & Schelling, G. (2010). Motion sickness, stress and the endocannabinoid system. PloS one, 5(5), e10752.
- Pisani, A., Fezza, F., Galati, S., Battista, N., Napolitano, S., Finazzi‐Agrò, A., … & Maccarrone, M. (2005). High endogenous cannabinoid levels in the cerebrospinal fluid of untreated Parkinson’s disease patients. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society, 57(5), 777-779.
Further Reading







User Guide, CBD, Dosage
CBD Dosage Calculator: How Much CBD Should I Take?
Further Reading
CBD, CBD Oil, Health, Health Benefits
55 Evidence-Based Benefits of CBD Oil (Plus Side-Effects)